⭐INTRODUCTION
Skin pigmentation disorders are among the most common concerns in dermatology. Changes in skin color—either lighter (hypopigmented) or darker (hyperpigmented) patches—can result from a wide range of causes. Understanding their differential diagnosis is essential for accurate treatment and management.
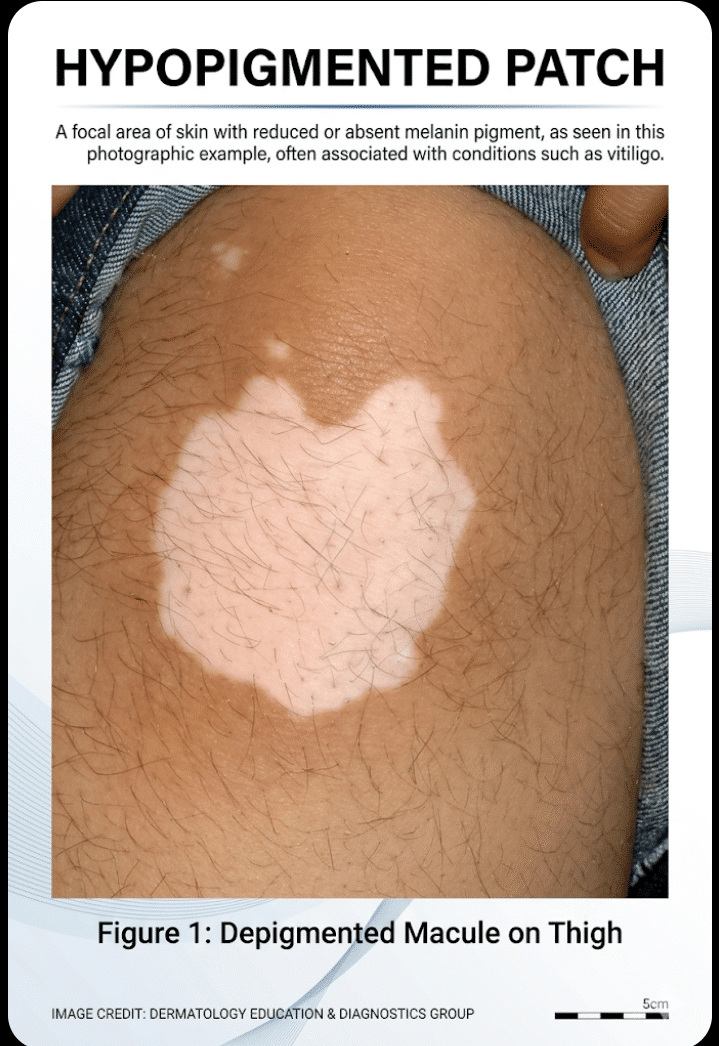
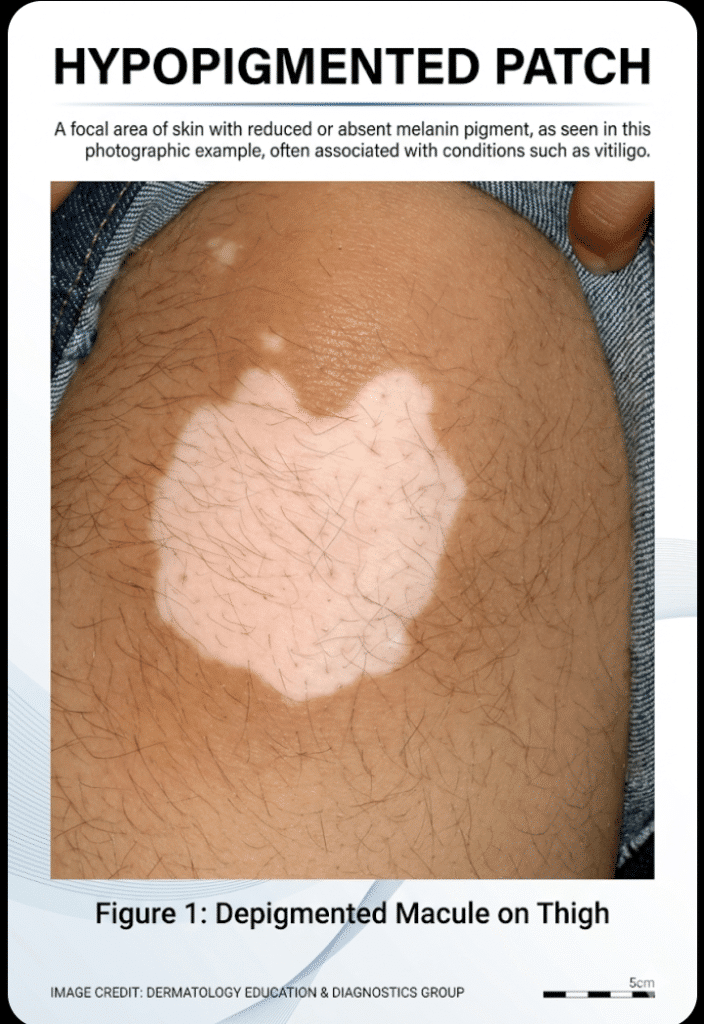
🌿 Hypopigmented Patches (Light-Colored Areas)
🔍 Common Causes & Differential Diagnosis
- Milky-white patches with well-defined borders
- Often symmetrical
- Common on face, hands, genitals
- Autoimmune destruction of melanocytes
- Caused by Malassezia fungus
- Fine scaling, mild itching
- Common on chest, back, shoulders
- Patches may be lighter or darker
- Ill-defined, dry patches
- Common in children
- Usually on cheeks and arms
- Associated with dryness and mild eczema
- Hypopigmented patches with loss of sensation
- Nerve thickening may be present
- Requires early diagnosis and treatment
- Post-Inflammatory Hypopigmentation
- Occurs after burns, infections, or skin inflammation
- Temporary or permanent
⚠️ Key Clinical Clues
- Sharp borders + no scaling → Vitiligo
- Fine scaling + mild itch → Fungal infection
- Loss of sensation → Leprosy
- Dry skin in children → Pityriasis Alba
🌞 Hyperpigmented Patches (Dark-Colored Areas)
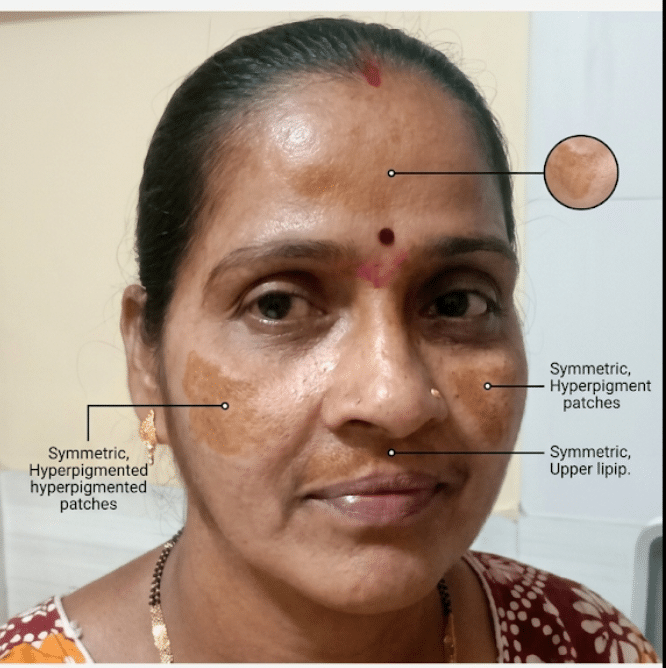
HYPERPIGMENTED PATCH
🔍 Common Causes & Differential Diagnosis
- Symmetrical brown patches
- Common in women
- Triggered by sun exposure, hormones
- Post-Inflammatory Hyperpigmentation (PIH)
- Follows acne, burns, or injuries
- More common in darker skin types
- Dark, thickened, velvety skin
- Common on neck, axilla
- Associated with diabetes/obesity
- Violaceous (purple) lesions
- May leave hyperpigmented marks after healing
- Drug-Induced Pigmentation
- Caused by medications like antimalarials, minocycline
⚠️ Key Clinical Clues
- Symmetrical facial patches → Melasma
- Velvety thick skin → Acanthosis Nigricans
- After injury/acne → PIH
- Purple lesions → Lichen Planus
🧪 Approach to Diagnosis
- Detailed history (onset, duration, drug use, sun exposure)
- Clinical examination (distribution, scaling, sensation)
- Wood’s lamp examination
- Skin scraping (KOH test) for fungal infection
- Biopsy in doubtful cases
❓ Frequently Asked Questions (FAQ)
1. Are hypopigmented patches always serious?
No. Many are harmless (like pityriasis alba), but some (like leprosy) need urgent care.
2. Can hyperpigmentation go away on its own?
Yes, especially post-inflammatory types, but it may take months.
3. Is vitiligo contagious?
No, vitiligo is an autoimmune condition and not infectious.
4. How can I differentiate fungal infection from vitiligo?
Fungal patches usually have scaling and itching, while vitiligo is smooth and non-itchy.
5. Does sun exposure worsen pigmentation?
Yes, it can worsen both melasma and contrast in vitiligo.
🧾 Conclusion
Hypopigmented and hyperpigmented patches have diverse causes, ranging from benign conditions to systemic diseases. A careful clinical evaluation, supported by appropriate investigations, is key to accurate diagnosis. Early recognition not only ensures effective treatment but also prevents complications and improves cosmetic outcomes.
👉 If you notice any unusual skin changes, especially persistent or spreading patches, consulting a dermatologist is always the best step.


